For Clinicians | Traveling With Medical Supplies Getting Weeks of Supplies Where Your Patient Is Going By Dr. Jamie Wilkey, PharmD — Director of Clinical Strategy, JaseMedically reviewed by Kristen Carpenter, PA-C — Clinical Advisory Board Member "My mother-in-law has...
The Search Bar Isn’t a Doctor

The Search Bar Isn’t a Doctor:
Why Medically Reviewed Medication Cards Matter
By Cayla McGrath
It’s 2 a.m. Urgent care closed an hour ago, your doctor’s office won’t reopen until morning, and whatever is going on feels miserable enough that sleep isn’t happening. Maybe it’s the familiar burning sensation of a urinary tract infection you’ve had before. Maybe your child woke up sick while you’re traveling three days from the nearest clinic. Maybe you’re riding out a hurricane, roads are flooded, and getting to a pharmacy simply isn’t an option.
For many people, moments like these end the same way: opening a search bar.
Or opening the medicine cabinet.
You find three leftover azithromycin tablets from a previous illness and wonder if they’ll work. You type your symptoms into an online symptom checker. You search social media. You text a friend who’s “good with medical stuff.” The reality is that when access to healthcare disappears, most people don’t do nothing. They do something.
At Jase, we think it’s important to acknowledge that reality.
We’re not teaching people to self-diagnose, and we’re certainly not encouraging people to play doctor. But we also recognize that the standard advice most patients receive — “Don’t self-treat. See a provider.” — quietly assumes a provider is reachable. It assumes cell service works, urgent care is open, your physician is available, and the nearest pharmacy isn’t two counties away after a disaster.
Sometimes, those assumptions simply aren’t true.
The question then becomes less about whether someone will make a decision and more about what information they’ll use to make it. Will it come from an algorithm designed to keep you clicking? Will it come from a decade-old forum post? Will it come from whatever antibiotics happen to be left in the back of a medicine cabinet?
Or will it come from clinicians?
Interestingly, medicine already acknowledges that there are situations where guided self-treatment makes sense when access is the limiting factor. The CDC’s Yellow Book recommends standby treatment for travelers carrying antibiotics to self-treat moderate or severe travelers’ diarrhea. The American Urological Association supports self-start therapy for select patients who experience recurrent urinary tract infections. Wilderness medicine experts have long recommended that expedition medical kits include medications clearly labeled with indications, dosing instructions, warnings, and circumstances that require evacuation or professional care.
The common thread isn’t encouraging people to guess.
It’s providing guardrails.
Because intuition can be both remarkably accurate and surprisingly unreliable. Research suggests that women with recurrent, culture-confirmed urinary tract infections identify new infections with better than 85 percent accuracy. At the same time, studies suggest only about one in nine women correctly identify a classic yeast infection based on symptoms alone.
Both of those facts can be true.
People often know when something feels familiar. What they may not know is whether the medication they’re considering is the right one, what dose should be taken, how long it should be used, whether there are situations where it should be avoided entirely, or when symptoms have crossed the threshold from “reasonable contingency plan” to “you need medical evaluation.”
That’s exactly why Jase created medically reviewed medication cards.
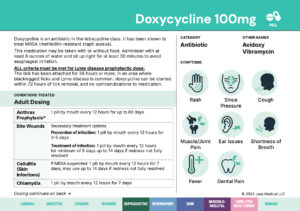
Rather than asking patients to rely on memory or internet searches, the cards provide condition-specific guidance developed and reviewed by medical doctors, physician assistants, and pharmacists. Each card outlines the medication itself, recommended dosing, duration of use, common side effects, situations where the medication should not be taken, and signs that indicate someone should seek professional medical care instead.
In many ways, the cards spend just as much time talking about limitations as they do permissions. They don’t say, “You’re on your own.” They say, “Here’s what clinicians want you to know if you’re ever in a situation where we can’t immediately be reached.”
The visual itself makes the argument. Instead of relying on guesswork, patients have plain-language guidance already in their hands: the right drug, the right dose, the right duration, when to avoid taking it, and when to stop and seek care instead. For someone who is traveling, weathering a disaster, or facing a 2 a.m. moment without access to healthcare, that distinction matters.
For us, that’s what appropriate medical preparation really means.
It isn’t replacing your primary care physician. It isn’t encouraging people to diagnose complex illnesses at home. It isn’t stockpiling medications for every imaginable scenario.
It’s recognizing that life doesn’t always happen within business hours.
Travel happens. Storms happen. Disasters happen. Backcountry trips happen. Phones lose signal. Clinics close. Pharmacies run out of medications.
And when those moments come, we’d rather people have clinician-written guidance in their hands than a search bar on their screen.
That’s not permission to guess.
It’s permission to be thoughtfully prepared.
At Jase, we call that appropriate medical preparation.
Cayla McGrath is a content strategist with Jase Medical. This post is for informational purposes only and does not constitute medical advice. Always consult a licensed healthcare provider before using any prescription medication.
Lifesaving Solutions
Everyone should be empowered to care for themselves and their loved ones during the unexpected. Check out our recent lifesaving products today.
Recent Posts
Keeping you informed and safe.

For Clinicians | Traveling With Medical Supplies
read more

The Search Bar Isn’t a Doctor
The Search Bar Isn't a Doctor: Why Medically Reviewed Medication Cards Matter By Cayla McGrath It's 2 a.m. Urgent care closed an hour ago, your doctor's office won't reopen until morning, and whatever is going on feels miserable enough that sleep isn't...

For Clinicians | Standby Antibiotics and Self-Start Therapy
For Clinicians | Standby Antibiotics and Self-Start Therapy Guideline Case for Guided Self-Treatment By Dr. Jamie Wilkey, PharmD — Director of Clinical Strategy, JaseMedically reviewed by Kristen Carpenter, PA-C — Clinical Advisory Board Member Patients stopped asking...

What Actually Happens When Medications Expire — And When It Matters
What Actually Happens When Medications Expire And When It Matters By Cayla McGrath If you've ever stood in front of your medicine cabinet holding a bottle a year past the printed date, wondering whether to toss it or keep it, you already know there are exactly two...