
For Clinicians | Standby Antibiotics and Self-Start Therapy
Guideline Case for Guided Self-Treatment
By Dr. Jamie Wilkey, PharmD — Director of Clinical Strategy, Jase
Medically reviewed by Kristen Carpenter, PA-C — Clinical Advisory Board Member
Patients stopped asking me whether they should keep leftover antibiotics years ago. They just tell me they did, usually after the fact, usually at the counter, usually with a little defiance in it: their old azithromycin from last winter went toward what felt like a UTI, aaaand they’re only bringing it up now because the symptoms didn’t budge.
Wrong drug for the likely bug. Wrong duration even if it were the right one. And the standard answer we’re all trained to give: “never self-treat, see a provider!” was never really in the running. It assumes a provider was reachable, and at 2am with no cell service, or three days out from the nearest clinic, nobody is. Patients in those moments will act on something. The only question is whether that something was written by clinicians, by a search bar, or just what is at the back of the medicine cupboard.
So today we’re going to flesh this out: what the guidelines already permit, where patient self-diagnosis is reliable (and where it really isn’t), what patients actually do when they can’t reach us, and what the guidance in their hands should look like.
Can patients accurately self-diagnose?
It depends on the condition, and the spread is wider than most of us would guess.Let’s just start at the encouraging side. In women with prior culture-confirmed UTIs, patient suspicion of a new UTI is more than 85% accurate in predicting culture-positive infection, more accurate than a urine dipstick.¹ This holds for women with an established recurrent pattern whose symptoms match prior confirmed episodes, and accuracy drops when vaginal discharge, pelvic pain, or STI exposure complicates the picture. But within those bounds, these patients know their bodies, and the data backs them.Now the other end. When women self-diagnosed a yeast infection and bought an over-the-counter antifungal, only about one in three actually had vulvovaginal candidiasis. The rest had bacterial vaginosis, mixed vaginitis, trichomoniasis, or normal findings. A prior clinician-confirmed yeast infection did not make them any more accurate the second time.²Hold both results at once. Patient intuition is real, and it is not uniform. It is condition-dependent, and patients have no way of knowing which conditions their intuition is good for. That specificity gap is exactly what a written tool has to close.
The permission already exists
The reflex is to file guided self-treatment under fringe medicine. The guidelines disagree.
- Recurrent UTIs. The AUA’s guideline lets clinicians offer select patients self-start therapy: the antibiotic waits at home, and the patient starts it when symptoms hit.³
- Travelers’ diarrhea. The CDC Yellow Book tells travelers to carry an antibiotic and start it themselves when moderate-to-severe symptoms hit. No call required.⁴
- Expedition medicine. Kits are scaled to how far the group is from care, and every drug is labeled with what it treats and how to take it.
- Your own exam room. We already prescribe ahead of the emergency: EpiPens, rescue inhalers, nitroglycerin. The patient carries the drug and uses their own judgment on the day.
Every one of these kicks in when care is out of reach. And every one of them assumes a clinician is nearby doing the guiding.
That’s the gap. We trained inside a closed system: one patient, one prescriber, one chart, one pharmacy. Nobody trained us for the patient at 2am, because she was supposed to be somebody else’s problem. There is no somebody else at 2am except maybe an ultra expensive ER with a wait a mile long. The permission for guided self-treatment exists. The plain-language tool it assumes was never built.
What medically-reviewed guidance actually looks like
This is where the med card earns its place, and the card makes the argument better than any abstraction does. Take the doxycycline card that ships in a JaseCase. The front opens with the counseling we give at the counter (take it with a full glass of water and stay upright for 30 minutes, your esophagus will thank you), then a conditions-treated table with adult dosing for each indication. The doses are not interchangeable: a single two-pill dose for Lyme prophylaxis, twice daily for 10 days for tetanus, once daily starting before travel for malaria prevention, up to 60 days for anthrax. They differ by condition, which is precisely what patients guess wrong. And the Lyme line won’t even grant that single dose unless every criterion is met: tick attached 36 hours or more, a region where blacklegged ticks are common, started within 72 hours of tick removal, no contraindications. That’s the IDSA’s own prophylaxis standard, printed where the patient can read it.⁷
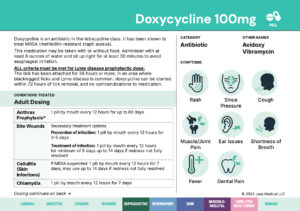

The back carries the side effects worth watching for, when to avoid the drug entirely, and a red Pregnancy Category D where nobody can miss it. Scattered through the dosing table is a phrase doing quiet stewardship work: secondary treatment option. The card tells the patient when this drug is not the right first choice. For pneumonia it goes further and requires a second antibiotic alongside it, partner drug and dose spelled out: the same combination the ATS/IDSA pneumonia guideline recommends for outpatients with comorbidities.⁸ That is the part the skeptics skip: the card spends as much ink on limits as on permissions.
The stewardship objection deserves a direct answer
The strongest pushback on at-home antibiotic kits, and infectious disease colleagues have made it in print, is antimicrobial resistance: patients shooting from the hip with broad-spectrum drugs. The concern is legitimate, and it deserves engagement rather than a dodge.
But look at what the objection assumes: that the alternative to the kit is a clinic visit. For the no-access moments these kits exist for, it isn’t. The real alternatives are going without, taking whatever antibiotics turn up around the house or from a friend’s leftover stash, or buying whatever they think they need from an online pharmacy. None of those comes with the right spectrum, a full course, or any counseling behind it. Against that baseline, a condition-specific, full-course, clinician-reviewed regimen with explicit do-not-use guidance is better stewardship, not worse.
And sometimes the right answer on the card is no drug at all. The clinical review behind each card draws the fence deliberately: well-understood, self-limiting conditions with predictable treatment paths, screened ahead of time by a clinician who reviewed the patient’s history. That fence is what keeps guided self-treatment from sliding into the free-for-all the skeptics fear.
Charting the grey area in public
Step back and look at how antibiotic access actually works in this country. It is all or none. Either the patient reaches a prescriber and gets the right drug, or they are completely on their own resources: the leftover stash, the search bar, the no-questions-asked website. There is no sanctioned middle step. We built a light switch and then act surprised when patients in the dark go looking for matches.
The guidelines covered above have already sketched what the middle step looks like: a defined, conditional, clinician-controlled layer between “call your doctor” and “you’re on your own.” Self-start therapy is that layer for recurrent UTIs. Standby treatment is that layer for travelers. What we’re building at Jase is the same layer for a short list of common, well-understood infections: the clinical work happens up front, a clinician reviews the patient’s history and prescribes for defined conditions, and the card carries the guidance into the moment it’s needed. That is what appropriate medical preparation means in practice: the basics, decided ahead of time, for the moments care isn’t there.
The boundary holds on both sides. This is in no way a replacement for primary care: anything complex, chronic, or unfamiliar still belongs in the exam room, and the cards say so. And if a patient asks you what they should have on hand just in case and you would rather not chart that middle layer yourself, you can refer them to us at Jase.com. We’re a family team of physicians, PAs, and pharmacists drawing these lines carefully, and we’ll keep publishing where we draw them.
The bottom line
Organized medicine already endorses guided self-treatment when access is the constraint; the existing frameworks just assume a clinician is standing there to do the guiding. At 2am, nobody is. What we can control is whether the information in the patient’s hand that night came from clinicians or from a search bar.
Most people never think about any of this until the night it happens to them.
We are here for them then.
Sources
- American Family Physician (AAFP), April 2016. Patient suspicion of UTI is more than 85% accurate in predicting culture-positive infection, more accurate than urine dipstick. https://www.aafp.org/pubs/afp/issues/2016/0401/p560.html
- Ferris DG, et al. Obstetrics & Gynecology, 2002. Among women who self-diagnosed vulvovaginal candidiasis and purchased an over-the-counter antifungal, 33.7% had the condition. https://pubmed.ncbi.nlm.nih.gov/11864668/
- AUA/CUA/SUFU, Recurrent Uncomplicated Urinary Tract Infections in Women, 2025 guideline amendment. Patient-initiated (self-start) treatment for select patients, conditional recommendation (Moderate, Grade C). https://www.auanet.org/guidelines-and-quality/guidelines/recurrent-uti
- CDC Yellow Book, Travelers’ Diarrhea. Standby self-treatment for travelers; antibiotics reduce illness duration by approximately 1 to 2 days for susceptible bacterial pathogens. https://www.cdc.gov/yellow-book/hcp/preparing-international-travelers/travelers-diarrhea.html
- IDSA/AAN/ACR, Prevention, Diagnosis and Treatment of Lyme Disease guideline, 2020. Single-dose doxycycline prophylaxis within 72 hours of a high-risk bite: identified Ixodes vector, highly endemic area, attached 36 hours or more. https://www.idsociety.org/practice-guideline/lyme-disease/
- ATS/IDSA, Community-Acquired Pneumonia guideline, 2019, summarized in American Family Physician, 2020. Outpatients with comorbidities: amoxicillin/clavulanate plus a macrolide or doxycycline. https://www.aafp.org/pubs/afp/issues/2020/0715/p121.html
Lifesaving Solutions
Everyone should be empowered to care for themselves and their loved ones during the unexpected. Check out our recent lifesaving products today.
Recent Posts
Keeping you informed and safe.

For Clinicians | Doxycycline Uses
For Clinicians | Doxycycline Uses Lyme Prophylaxis, Malaria Prevention, Acne, and the Doxy-PEP Debate By Dr. Jamie Wilkey, PharmD — Director of Clinical Strategy, JaseMedically reviewed and edited by Kristen Carpenter, PA-C We're continuing our series on the...

For Clinicians | The Family Emergency Plan Checklist
For Clinicians | The Family Emergency Plan Checklist The Medical Layer Most Plans Miss By Dr. Jamie Wilkey, PharmD — Director of Clinical Strategy, JaseMedically reviewed and edited by Aaron Asay, PA-C, DMSc, FIBODM, FAWM When disaster strikes, medical personnel in a...

Food Poisoning vs. Stomach Infection
Food Poisoning vs. Stomach Infection Three Different Stomach Bugs. Three Different Answers to 'Do I Need Antibiotics? By Cayla McGrath 'Food poisoning,' 'stomach flu,' and 'stomach infection' get treated as essentially the same thing — and the prescription question...

For Clinicians | Food Poisoning, Stomach Flu, or H. Pylori
For Clinicians | Food Poisoning, Stomach Flu, or H. Pylori Do You Actually Need Antibiotics? By Dr. Jamie Wilkey, PharmD — Director of Clinical Strategy, JaseMedically reviewed by Kristen Carpenter, PA-C — Clinical Advisory Board Member Three patients, same complaint....