
For Clinicians | Azithromycin (Z-Pack)
Why It Earns a Place in Appropriate Medical Preparation
By Dr. Jamie Wilkey, PharmD — Director of Clinical Strategy, Jase
Edited and approved by Kristen Carpenter, PA-C — Clinical Advisory Board Member
Can’t you just call in a Z-Pack?“
Your patients probably ask for one all the time. They know it works, and almost everyone has taken one at some point in their life.
Today we’re talking about the Z-Pack and why it’s so helpful for appropriate medical preparation across a number of different common conditions. What it’s approved to treat. What it’s actually being used for. And where the line sits between what’s okay for a patient to keep on hand and what still needs to be seen by a doctor.
What is azithromycin, and what does it treat?
Azithromycin is a macrolide antibiotic, FDA-approved for a number of common bacterial infections.¹ Most courses run 3 to 5 days, with one-time single-dose regimens for a few specific indications.
A few things make it useful when access to care is delayed:
- The course is short. The drug accumulates in tissue and has a prolonged terminal half-life, which clinically supports a short course providing antimicrobial activity beyond the dosing window.²
- It covers the common community-acquired pathogens behind respiratory infections, skin and soft tissue infections, certain sexually transmitted infections, and traveler’s diarrhea.¹
- It’s a real option for patients who can’t take penicillin, which is a larger group than most clinicians realize.
- It’s oral, well-tolerated, and inexpensive.
FDA-approved indications include:¹
- Acute bacterial sinusitis
- Acute bacterial exacerbation of chronic bronchitis (mild to moderate)
- Community-acquired pneumonia (mild severity, suitable for outpatient oral therapy)
- Pharyngitis and tonsillitis as an alternative to first-line therapy in penicillin-allergic patients
- Uncomplicated skin and skin structure infections
- Urethritis and cervicitis due to Chlamydia trachomatis or certain gonococcal infections
- Genital ulcer disease due to chancroid
- Acute otitis media in pediatric patients
Guideline-supported uses outside the FDA label:
- Traveler’s diarrhea, particularly in regions where fluoroquinolone-resistant Campylobacter is common (notably Southeast Asia).³
- Pertussis treatment and post-exposure prophylaxis.⁴
- MAC prophylaxis in HIV patients with CD4 <50 not on effective ART, and as part of combination treatment for disseminated MAC.⁵
Why azithromycin is in the JaseCase
We here at Jase provide, ahead of time, the medications patients need for a number of emergencies, and azithromycin is one of our favorites.
When a patient picks up a prescription at their regular pharmacy, the clinical work has already been done: the diagnosis is confirmed, the indication is documented, the dosing is verified, and the pharmacist is two steps from the prescriber if anything looks off. Contingency stocking removes all of those backstops. The protocol, the indication match, the dosing, the dispensing instructions, and the patient education all have to be locked before the bottle goes on the shelf.
Jase is in a unique position to help patients proactively. We prescribe for a select set of emergencies, before they happen, at the same clinical standard a patient would receive in the room. Azithromycin earns its place in the JaseCase against a specific set of criteria for contingency use:
Indication breadth. One molecule covers the common community-acquired infections a patient is most likely to encounter outside business hours: a sinus infection that goes brutal on day three, a respiratory infection that won’t quit, a strep-positive kid who can’t take amoxicillin, a chlamydia exposure that needs treating, traveler’s diarrhea that hits halfway through a trip. Stocking one drug that addresses several presentations is more useful in a kit than stocking five drugs each addressing one.
Fixed, short dosing. A 3 to 5 day course with no titration, no renal dose adjustment in the typical adult, no requirement for serum levels, and no repeat dosing decisions. The course we wrote ends when the package ends.
Penicillin alternative. About 10% of the U.S. population carries a documented penicillin allergy on their chart.⁶ The true IgE-mediated rate is closer to 1%, but the labeled-allergy patients still avoid penicillin-class drugs in real practice because confirming the true rate requires testing most patients haven’t had. Amoxicillin-clavulanate is the other common kit antibiotic, and for roughly one in ten patients it isn’t an option. Azithromycin is.
Familiarity that reduces error. Roughly 10.3 million prescriptions for azithromycin are written every year in the U.S., making it the 64th most-commonly prescribed medication in the country.⁷ The patient has likely taken it. The prescriber writes it from muscle memory. The protocol Jase delivers with the kit slots into a pattern both already know. Familiar drugs are safer drugs in contingency use.
Storage and stability. Tablets, room temperature, multi-year shelf life. The drug stays viable in a kit on a shelf at home or in a glovebox on the road.
This is how we treat all the drugs in our JaseCase. They’re very carefully selected.
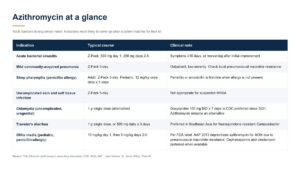
Azithromycin at a glance
The view for the indications most likely to come up when a patient reaches for their kit. Doses are adult standard unless noted.
Don’t reach for azithromycin for:
- Viral upper respiratory infections. Antibiotics don’t help. Symptomatic care.
- Suspected gonorrhea. CDC now recommends ceftriaxone monotherapy; azithromycin is no longer routinely added.⁸
- Suspected MRSA skin or soft tissue infections.
- Anything escalating: high fever, sepsis signs, immunocompromise, hemodynamic instability, or systemic involvement.
- Bacterial infections where a beta-lactam is first-line and the patient is not actually penicillin-allergic. Use the right tool.
Two cautions worth flagging:
- QT prolongation. Use caution in patients with known QT prolongation, electrolyte derangements, or concurrent QT-prolonging medications.⁹
- Macrolide resistance. Pneumococcal macrolide resistance is significant and varies by region. For pneumonia in particular, current resistance patterns matter for empiric choice.
Stewardship is the bar, not the brake
The answer is the clinical work that happens before the bottle ever ships, while the situation is still calm and considered. For contingency stocking, the prescriber isn’t going to see the patient at the moment of use, so the screening has to be stricter on the front end, not looser. We review the patients current medical conditions, medications, and any allergies they may have to determine if the case medications would be safe for them to take. Patients complete an intake and attestations, a licensed prescriber reviews them against those criteria, and the kit ships only when the fit is appropriate. The patient isn’t reaching into the cabinet on instinct. They are reaching for a medication a prescriber already cleared for them, before they ever got sick.
Each medication in the kit ships with an information sheet: basic drug information, common side effects, contraindications, and dosing for common conditions. The sheets aren’t a diagnostic tool. They are reference materials patients can use to follow the prescriber’s plan and bring accurate information into the room if they end up in front of another clinician. Our team can answer clarification questions about how the medications work. We are not the patient’s treating clinician, and the kit is not a substitute for primary care.
Contingency stocking in this category needs to clear a higher stewardship bar than routine office prescribing, not a lower one. The patient is going to be at home, at a campsite, on a cruise ship, in a hotel halfway across the world, somewhere the prescriber can’t see them. That changes the protocol design. It does not relax it.
Who makes these calls
Our team is medical doctors, physician assistants with field experience in disaster medicine and humanitarian response, and pharmacists. The clinical work happens on the front end, so the patient isn’t doing it alone at 11pm.
Kristen Carpenter, PA-C, put it this way when we mapped out the JaseCase formulary:
“When we decided which antibiotics belonged in the JaseCase, azithromycin was an easy choice. It’s a broad-spectrum antibiotic that can treat a number of different bacterial infections. It is fast acting, usually requires shorter treatment courses, compared to other antibiotics, and is a great alternative for people who are allergic to, or cannot get, penicillin, offering a necessary backup in a limited-supply scenario.“
Charting the grey area in public
Contingency stocking for predictable, common emergencies is a real clinical category, and the guidelines haven’t caught up to it yet. Our team is publishing how we make these calls, the criteria we use to add or exclude a drug, and the protocols we deliver with each kit.
If a patient keeps asking and you’d rather not take on the contingency work yourself, you can refer them to us at Jase.com. It’s a clinical handoff, not a product pitch.
Public knowledge gets better when clinicians chart the grey area in public instead of letting the internet do it. The category is going to fill in. The question is who fills it in, and with what standard.
The bottom line
Azithromycin earned its place in the JaseCase on clinical merit: indication breadth, short fixed-course dosing, a real penicillin alternative, familiarity, and shelf stability. The same screen applies to every drug we add. This is not a replacement for primary care. It is the bridge for the moments primary care isn’t there. Trusted medicine, on your patient’s shelf, before the moment they need it.
To learn more, check us out at Jase.com.
Sources
- FDA Zithromax (azithromycin) prescribing information. Indications and Usage; Dosage and Administration. DailyMed: https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=db52b91e-79f7-4cc1-9564-f2eee8e31c45
- FDA Zithromax (azithromycin) prescribing information, Clinical Pharmacology section (pharmacokinetics: tissue distribution and prolonged terminal half-life). Same DailyMed reference as #1.
- CDC Yellow Book, Travelers’ Diarrhea chapter. Azithromycin first-line empiric treatment in Southeast Asia and other regions with fluoroquinolone-resistant Campylobacter. https://www.cdc.gov/yellow-book/hcp/preparing-international-travelers/travelers-diarrhea.html
- CDC. Pertussis (Whooping Cough): Treatment and Post-Exposure Prophylaxis. https://www.cdc.gov/pertussis/hcp/clinical-care/index.html (treatment overview); https://www.cdc.gov/mmwr/pdf/rr/rr5414.pdf (MMWR RR-54/14, 2005, for dosing).
- NIH/CDC/IDSA. Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV: Mycobacterium avium Complex. Azithromycin is the preferred agent for primary prophylaxis (CD4 <50 not on effective ART) and a preferred first agent as part of combination treatment for disseminated MAC. https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-opportunistic-infections/disseminated
- CDC. Evaluation and Diagnosis of Penicillin Allergy for Healthcare Professionals. ~10% of U.S. patients report a penicillin allergy; <1% are truly allergic. https://www.cdc.gov/antibiotic-use/hcp/clinical-signs/index.html. Supporting: Castells M, Khan DA, Phillips EJ. “Penicillin Allergy.” N Engl J Med 2019;381:2338-2351.
- ClinCalc DrugStats Database. Azithromycin: estimated 10,337,595 U.S. prescriptions (2023), ranked #64 among the most-commonly prescribed medications. https://clincalc.com/DrugStats/Drugs/Azithromycin
- CDC Sexually Transmitted Infections Treatment Guidelines, 2021. Gonococcal infections: ceftriaxone monotherapy (500 mg IM single dose for patients <150 kg). Azithromycin is no longer routinely added to dual therapy. Chlamydial infections: doxycycline 100 mg BID x 7 days is the recommended regimen; azithromycin 1 g single dose is listed as an alternative. https://www.cdc.gov/std/treatment-guidelines/gonorrhea-adults.htm and https://www.cdc.gov/std/treatment-guidelines/chlamydia.htm
- Ray WA, Murray KT, Hall K, Arbogast PG, Stein CM. “Azithromycin and the Risk of Cardiovascular Death.” N Engl J Med 2012;366:1881-1890. FDA Drug Safety Communication, March 2013: azithromycin QT prolongation risk. https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-azithromycin-zithromax-or-zmax-and-risk-potentially-fatal-heart. Current Zithromax label includes QT prolongation in Warnings.
Lifesaving Solutions
Everyone should be empowered to care for themselves and their loved ones during the unexpected. Check out our recent lifesaving products today.
Recent Posts
Keeping you informed and safe.

Measles, Dengue, and the World Cup: The 20-Minute International Travel Checklist We Use Before Every Trip
Measles, Dengue, and the World Cup: The 20-Minute International Travel Checklist We Use Before Every Trip By Cayla McGrathEdited and approved by Kristen Carpenter, PA-C — Clinical Advisory Board Member For many soccer fans, attending the FIFA World Cup is a...

Can You Get Prescription Medication While Traveling Internationally?
Can You Get Prescription Medication While Traveling Internationally? By Cayla McGrathEdited and approved by Kristen Carpenter, PA-C — Clinical Advisory Board Member You're four days into a trip to Florence when the familiar symptoms start. You've had a urinary tract...

For Clinicians | World Cup 2026 Pre-Travel Counseling
For Clinicians | World Cup 2026 Pre-Travel Counseling Three Host Countries, Three Measles Outbreaks By Dr. Jamie Wilkey, PharmD — Director of Clinical Strategy, JaseEdited and approved by Kristen Carpenter, PA-C — Clinical Advisory Board Member By the time a patient...

For Clinicians | Can You Get Prescription Medication Abroad?
For Clinicians | Can You Get Prescription Medication Abroad? What Your Patients Assume, What's Actually True, and What to Do Before They Leave By Dr. Jamie Wilkey, PharmD — Director of Clinical Strategy, JaseEdited and approved by Kristen Carpenter, PA-C — Clinical...